Can HCD help bring humanity (back) to emergency response?
June 24, 2026

Alfred Kelfala from the roving Freetown Ebola burial team carefully places the body of an Ebola victim into a grave. photo: DFID – UK Department for International Development, CC BY 2.0
Note: This post is adapted from a talk “Adaptive SBC: Reaching People in Complex & Changing Contexts” given by Sherine Guirguis at SBCC 2026.
Every crisis has two stories: the one told by data, and the other one told by people. The story told by data is tidy, neatly organized in columns and rows, with a beginning and an end. But the messier stories told by people can last for generations; long after the reports have been finalized, and the response has packed up and moved on.
In October 2014, I went to Sierra Leone to support the largest and most complex Ebola outbreak the world has ever seen to date. By the time it was over, there were 28,000 reported cases and 11,000 deaths.
That’s the data story.
Here’s the human one.
In Sierra Leone, washing a dead body is about dignity, safe passage into the next world, and the transfer of power from the dead to the living. When you touch the deceased, you fulfill your obligation not only to your loved one, but also to your ancestors, and to the societies that have governed the passage between life and death for a thousand years.
But Ebola is most infectious at the moment of death — and the outbreak was tearing through the country, and the region faster and deadlier than anything anyone had ever seen before. In an attempt to curb the virus, the public health response forbade traditional funeral practices and burials.
Dead bodies were now being removed by strangers in hazmat suits within 24 hours. There was no washing, no gathering of loved ones, no goodbyes. No respects paid.
I arrived nine months into the outbreak, just after a single funeral in Moyamba district had been linked to 28 confirmed Ebola cases and 8 deaths.
The funeral was for a prominent pharmacist — a highly respected man whose passing required the proper rituals — washing, touching, gathering, mourning extended over many days; honoured by many people.
Once this was forbidden, families hid the dead bodies of their loved ones. They buried them at night. Moved their bodies in secret.
Public Health experts called that non-compliance. People called it a final act of love.
There’s a consistent narrative of noncompliance in every outbreak.
When people don’t follow public health directives, we assume they’re ignorant, or they don’t understand how the virus behaves. Ebola was a new disease in Sierra Leone – and it’s true that people didn’t fully understand the science behind it. But that’s not what this was. This was grief with nowhere to go. It was rage at being told that the most human thing you could do in the face of tragedy, was now forbidden.
For the vast majority of people, this new and unprecedented disease was scary, but the response ? That threatened to undo the fabric of their society. Among these two threats, the response was definitely scarier.
These were powerful human emotions at play.
But we responded to them the same way we responded to polio resistance in Pakistan, or frontline worker hostility in Nigeria, or rumors in DRC.
To public health responders, emotions are obstacles, irrational behavior rubbing up against scientific evidence, to be corrected with facts, science, and better information.
Our field has come a long way since 2014. We understand human behavior much better now. But we’ve remained almost exclusively focused on what people know. What they believe. What they intend to do. We are still not asking people how they feel.
And we don’t fully understand or appreciate how those feelings color everything else — the information they seek, how it’s interpreted, how it influences what they do.
We’ve all been part of decisions that are made inside an emotion. Anger changes what we hear. Fear changes what we see. Stress changes what feels possible. Grief can make even the most rational instruction feel impossible to follow.
Fast forward ten years — it’s 2024.
I’m now the co-founder of a behavioral design firm called Common Thread. My team is working on the Mpox response in Uganda and Burundi alongside UNICEF, and our challenge — on the surface — is familiar: how do we convince people to report mPox cases and come to treatment centers?
While my team was in the field, they came across half an Mpox poster that had been torn down at a case management centre in Kampala. As they walked through the centre, they saw another poster torn down, and then another, and another…. Healthcare workers told us that commercial sex workers had been tearing them down for some time.

But why?
The poster was factual and accurate. It looked helpful — it described transmission risks, symptoms to watch out for, and what to do if you thought you were infected. Exactly the kind of communication we reflexively produce to educate communities about an unknown disease, to reduce the fear.
By December 2024, Uganda had recorded 1,353 confirmed Mpox cases. Officially, sex workers accounted for 39 of them — less than 3% of the total.
Uganda’s Ministry of Health responded to this data by saying “zero-graze at home” — it was a term borrowed from the HIV/AIDS response, and it means, keep the livestock confined, stay faithful, don’t seek commercial sex. It was directed to male behaviour, but the stigma landed on women.
That poster, genuinely intended to inform people about Mpox, felt like a threat to sex workers, suggesting that their identity, their livelihood, their body is the vector.
Shame came next. Sex workers became reluctant to report their illness, making contact tracing harder. The very people the response needed to reach most became the hardest to find.
Here’s why this matters so much — and why I think it changes everything about how we design in emergencies.
When people are frightened, grieving, ashamed, overloaded, or trying to protect their family — the brain becomes less reflective. More protective. It relies less on slow, flexible thinking — what behavioral scientists call System 2 — and more on fast, familiar, automatic responses. System 1.
System 1 doesn’t weigh long-term risk vs benefit. A stressed brain doesn’t process new guidance or build trust with unfamiliar institutions. System 1 is designed to help us reflexively survive.
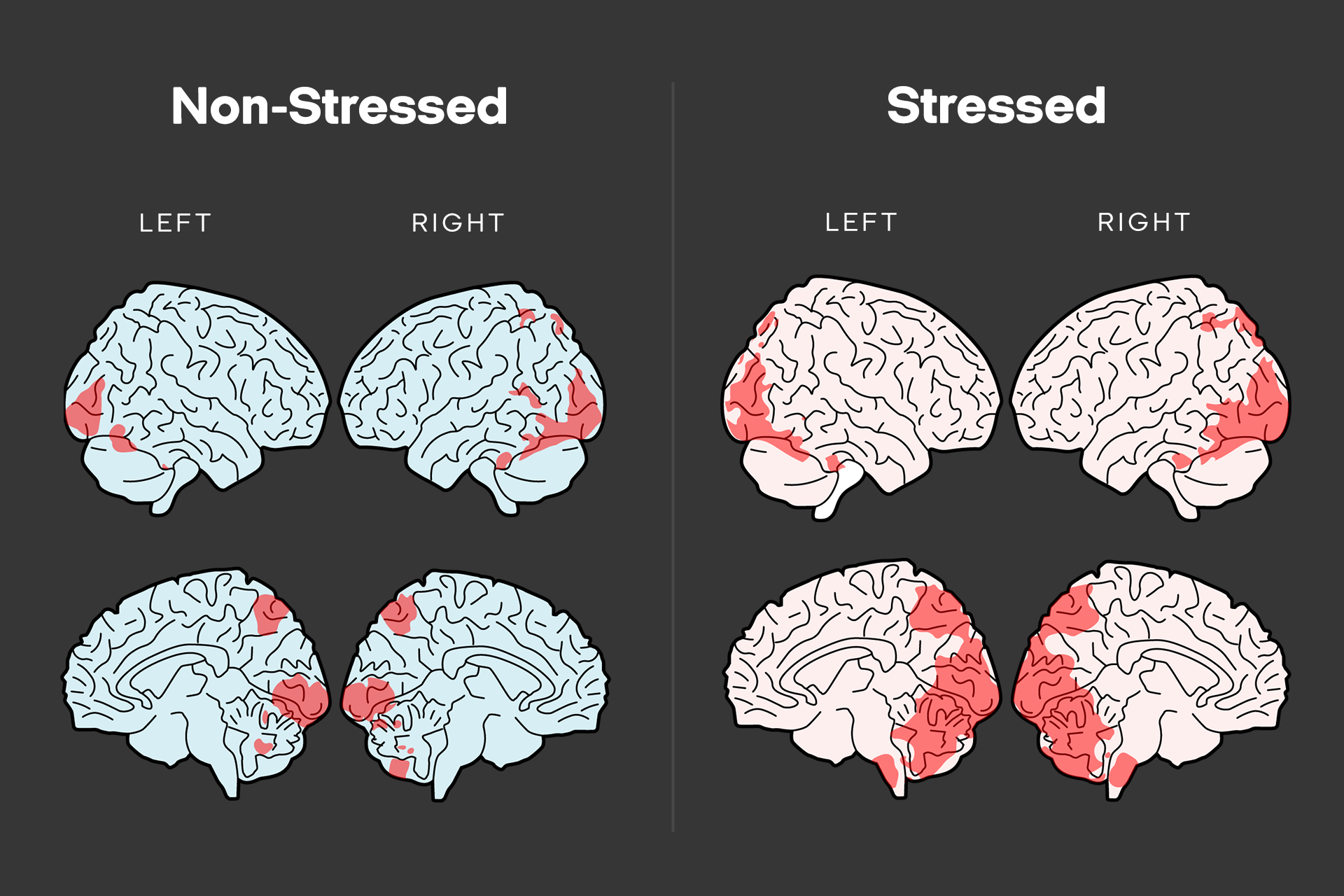
Adaptaed from Portes, B., Balardin, J.B., Lacerda, S. et al. The effects of perceived chronic stress on the fMRI correlates of attentional control in women managers. Arch Womens Ment Health 22, 375–381 (2019). https://doi.org/10.1007/s00737-018-0902-6
The irony of emergency response is that we ask people to do the most cognitively demanding things — understand a new disease, assess risk, trust strangers, change long-held practices — at the exact moment they have the least cognitive bandwidth to do it.
So when families hide their dead, when sex workers tear down posters — that isn’t ignorance or irrationality. That is a brain under stress doing exactly what it’s been wired to do: defaulting to what is familiar, and what feels protective.
In most emergencies, people are not failing to follow the public health response. The response is failing to fit the brain space people actually have.
This is where HCD comes in as such a powerful tool. And I want to argue for it not on moral grounds — though the moral case is strong — but on neurological and behavioral grounds.
HCD disrupts System 1 fight or flight thinking, not just in communities, but in responders and frontline workers. Because their brains are also in emergency mode. Responders default to assumptions, technical language, command-and-control habits. The response system has its own System 1. And I say “we” deliberately, because I’ve been a part of this. When System 1 kicks in, we stop asking questions. We execute. We produce posters. Jargon. Megaphones. Key messages. Reliably, and at speed.
At its core, HCD is a structured way of solving problems and designing solutions that puts people or human needs at the centre of every decision. HCD can help us ask: what does this problem feel like to you? And does the response make you feel more scared, ashamed, more stressed about your survival?
That is a completely different line of questioning from: Will you seek treatment if you become infected with this disease?
At Common Thread, we’ve been building something we think is missing from most behavioral frameworks. Together with our partners, we’ve been working on a new model of behaviour change — the Behavioural Pathways Model, that explicitly layers emotional states onto behavioral determinants.
The question we’re trying to ask is this: for any given behavior we’re trying to shift, what emotions are driving the person we’re trying to reach — and is that emotion conducive or obstructive to the behaviour in question?
A mother in Ituri right now knows exactly how Ebola spreads. She has a treatment centre within reach, and she will still hide her sick child. Because the fear of being unable to be with him at a treatment center will outweigh everything she knows. And the same fear cuts both ways: there’s another mother out there whose fear of the disease, and fear of her child’s death, will drive her towards care.
Our model forces us to design with the emotion in mind, not around it.
DRC is experiencing its seventeenth Ebola outbreak — except this time, there is no treatment and no vaccine. When people are looking around their communities, at healthcare workers in Hazmat suits, and posters on clinic walls, they’re implicitly asking: is this response for me or at me? They’re deciding, in milliseconds, whether to comply or resist. The design window isn’t when the poster goes up. It’s years before — in the relationships built, the trust earned, the feedback systems that were already listening.
If we don’t design for that emotional reality, every outbreak will cost us thousands of lives to learn, once again, those hard-won lessons we learned at the end of the West African outbreak. The lessons we learn at the end of every outbreak.
We have been part of that cycle. The entire public health sector has been part of that cycle.
Think back if you’ve sat in an emergency planning meeting where the response to “people aren’t following the guidance” or “doing the thing” or “coming for the treatment” was: Increase knowledge. Correct the myths. Write it better. Say it louder. Put up another poster. Go speak to the community — or get someone else to do it — so they do what we need them to do…
That was us in Sierra Leone in 2014. We wrote it. We sang it. We even danced it. We shouted it through megaphones. And the outbreak kept spreading, because we were all treating a frightened brain like a calm one, and a grieving family like a noncompliant one.
So here’s what I’m asking us all to do.
- Stop measuring only what people know and start measuring what they feel: build emotional data collection into your monitoring systems with the same rigor you give case counts. This needs money. It needs systems. It needs skills building.
- Let’s stop treating HCD as a luxury. An innovation we call when we’re stumped, and then rush it along. Instead, integrate it into a mindset for how you train health workers, how you design your monitoring systems, how you decide what counts as evidence, how you design the response. This work doesn’t start with an outbreak. It starts now — by building trust, building relationships. And it extends into an outbreak. If we do this, outbreaks will be shorter. They will be less deadly.
And try to remember, when you’re in the middle of a crisis, and your own brain is tired and operating under Sytem 1 — that the families hiding their dead, the sex workers tearing down posters, the mother who won’t bring her child in: none of that is irrational. It’s a brain doing exactly what it’s built to do under threat. It’s trying to survive. It has the same goal that you do.
So if there’s only one thing I hope you take away from this — it’s that emotions are not the irrational noise on top of rational decision-making. They are the decision-making.
Let’s design for that.