
Kenya
Call for Change Kenya: a new kind of innovation challenge
The Challenge
How might we understand and respond to the real needs of Kenyans amidst a global pandemic? (Spoiler alert: their real needs were not Covid-19)
This case study is Part 2 of 2 — For the first part of this project’s epic journey, read part 1 here.
When it comes to transforming public health, the problem isn’t usually a lack of imagination or ideas. Sometimes it’s a lack of connection.
Around the world, there are brilliant, community-led organisations with ideas rooted in lived experience. But these solutions are often sidelined by systems that favour top-down thinking, stringent reporting demands, and rigid global frameworks.
That was the central challenge we took on with Kenya’s Ministry of Health (MoH). This was no ordinary grant-making process. It was a co-designed journey that brought community-rooted organisations into direct partnership with government, creating new pathways for trust and visibility.
This case study shows how reducing friction for local partners to access funding, define their own priorities, and co-design their solutions together with local Governments can lead to smarter investments and lasting systems change.
The Backdrop: A Disconnect Between Priorities and Power
By late 2022, our research had shown that COVID-19 had largely faded as a top priority for most Kenyans. The country’s health system was strained by deadlier public health burdens like malaria and maternal health, but global funding still flowed toward pandemic response.
As one public health leader in Wajir said, “You cannot deliver COVID-19 vaccines across the country when many counties are still struggling to provide basics like mosquito nets or maternal care.”
Through interviews with donors, county officials, and local organisations, we learned that the deeper issue wasn’t resources, it was missed connections between data, people and resources. Local organisations had clear ideas, lived experience, and innovative strategies. But they didn’t have access to the data systems, coordination and resource support needed to act on them. Data flowed out of communities and into national and global databases, and stayed there. Donor requirements were rigid and hard for local, often-scrappy organisations to comply with. Proposal processes were arduous. And most funding still went to a narrow pool of known, well-resourced actors.
Rather than continue on the pandemic path, we began to help Kenya’s MoH strengthen their local health system so it could be more ready for the next shock. Business as usual was failing to include the best ideas and local talent, and we wanted to help shape a new way of working. One that made local leadership visible, trusted, and central.

Time to pivot
Covid-19 seemed like a drop in the ocean for Kenya’s health system, compared to challenges like malaria:
MALARIA VS. COVID-19, CONFIRMED CASES, 2022 (STATISTA):
Designing for Inclusion: Innovating the Innovation challenge
We could have taken two paths at this point: make a bunch of recommendations to the Ministry of Health and donors about what we thought should be done, or try something out and see if we could build a solution from the communities themselves. Could a local innovation challenge be the key? Maybe. But why haven’t they worked so far?
After reviewing over 20 different innovation challenges, we designed the Call for Change (CFC), an innovation challenge that applied behavioral science to de-bias the process. We stripped back the paperwork and invited anyone to submit a 250-word idea. No long forms and unnecessary requirements, just a social-media-friendly call to action.


Proposals were anonymised and reviewed using inclusive criteria: favouring locally- and women-led initiatives with strong community presence. Of the 29 final applications:
Targeted underserved or minority populations.
Were women-led or had a majority of women in program roles.
Were partnerships
sparked directly by
the CFC process





Idea Lab workshop in Nairobi

From Big Ideas to Local Change
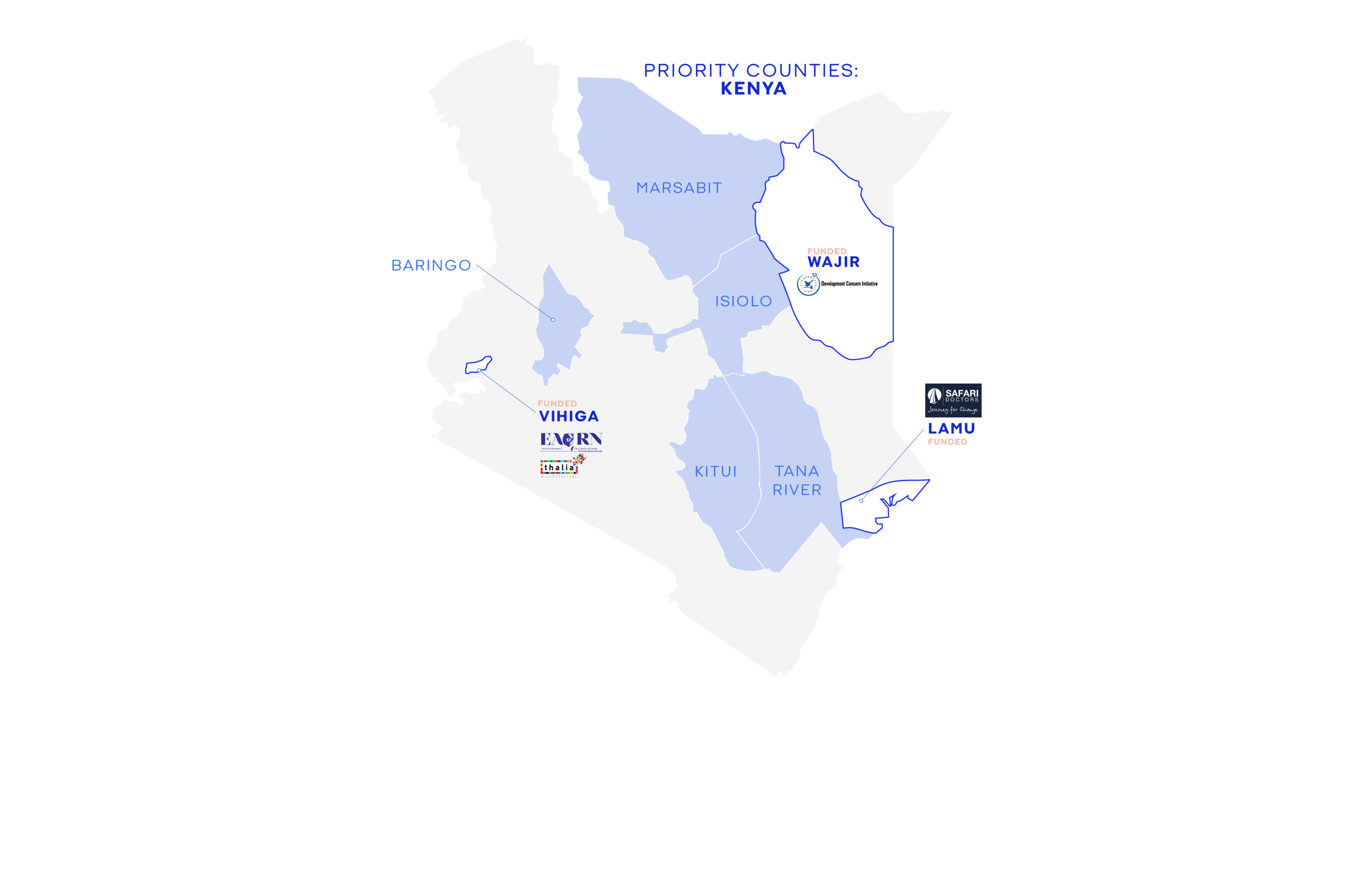
Four organisations received funding.
- Thalia Psychotherapy (Vihiga County) launched a pilot mental health program for healthcare workers. In six months, they reported a 30% increase in help-seeking behaviour and significant drops in burnout and absenteeism. Their work expanded into Uganda, Nigeria, and Ghana, and garnered national and international attention, including from WHO and Bloomberg.
- Development Concern Initiative (Wajir County) trained local Imams and women leaders to deliver health messages to nomadic communities. Their efforts enabled a coordinated response to a cholera outbreak and set a precedent for faith-based collaboration with government.
- Safari Doctors (Lamu County) created a network of Youth Health Ambassadors, trained and endorsed by elders, who brought health education and HPV vaccine awareness to hard-to-reach areas.
- Eastern Africa Child Rights Network (Vihiga County) co-designed health worker training with the County Health Management Team, leading to interest in national curriculum integration.
But that wasn’t even close to the end…
“The Call for Change has really awakened the real power of the population… together, the Department of Health, the women, other key stakeholders, together we have achieved so much.”
Project Manager, CFC-funded project

Redefining What It Means to “Win” A Challenge
All applicants, not just the ‘winners’, were integrated into a growing ecosystem of peer support, government collaboration, and shared learning. This community of practice became one of the most powerful legacies of the Call for Change.
Community members were given access to training in proposal writing and storytelling, and contributed to a collective learning journey. In 2025, this community remains active, sharing opportunities, tools, and ideas. The MoH joined as a participant, not just a sponsor. And a new open-access database now supports the MoH in identifying vetted, local partners.
Each funded project formalised partnerships with county governments, laying the groundwork for long-term sustainability. Local ownership was not symbolic — the MoH co-led every stage, from review to rollout.
Systems Change in Action
This journey wasn’t just about funding innovation. It was about proving that inclusive, participatory processes yield better solutions and that shifting power is not only possible, it works.
The Call for Change offers a blueprint: reduce friction, build trust, and design for equity. Let go of the instinct to control, and instead create space for community voices to lead.
Because when that happens, innovation doesn’t just scale. It sticks.
If you’re like us, and think Global Public Health might benefit from an equity-focused redesign, our Decolonisation Quizzes and Decolonization Playbook might be a good place to start.
This work was conducted in partnership with the Gates Foundation
